
The Glasgow Coma Scale (GCS) is an essential clinical tool used by healthcare professionals to assess and monitor a patient’s level of consciousness, particularly after a traumatic brain injury or other neurological impairments. Developed in 1974 by neurosurgeons Graham Teasdale and Bryan Jennett, the GCS provides a standardized method for evaluating a patient’s responsiveness in three key areas: eye opening, verbal response, and motor response.Respiratory Therapy Zone
The GCS evaluates three components:
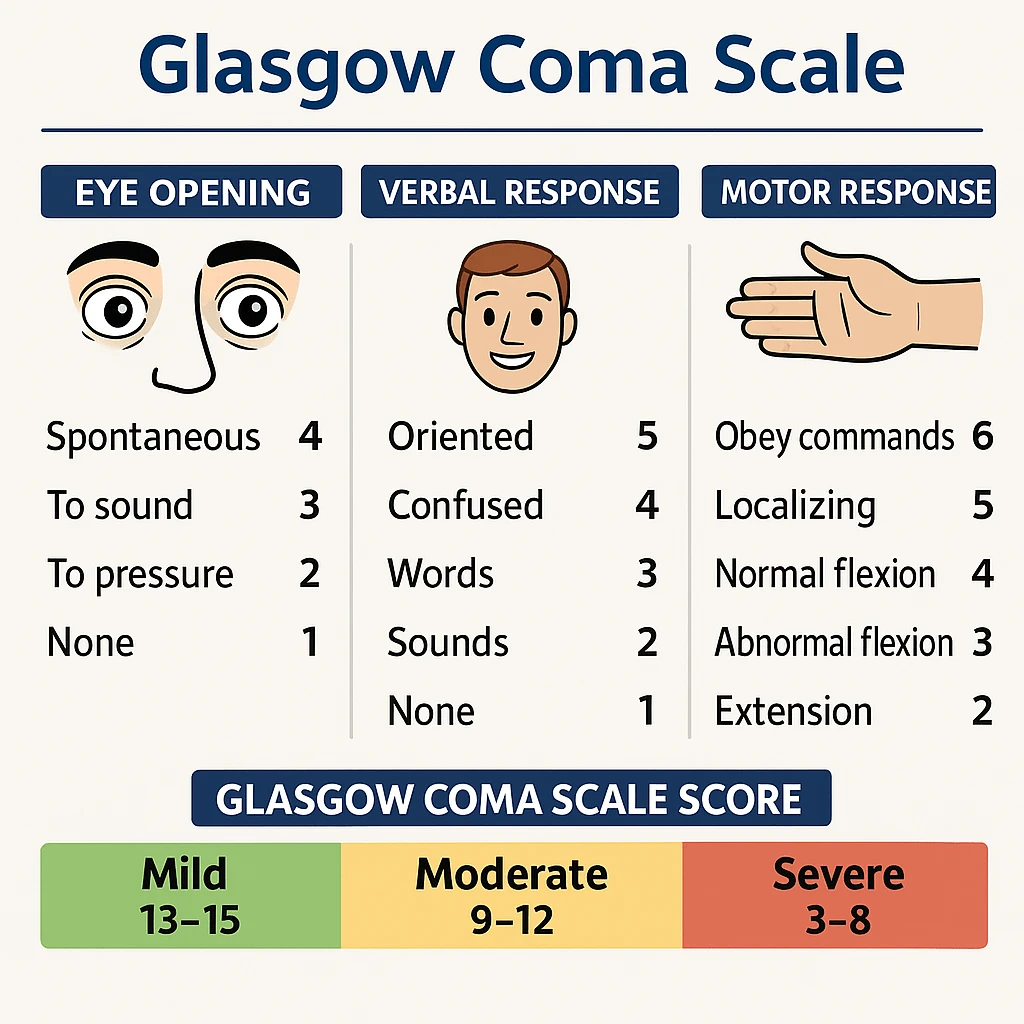
Eye Opening (E): Scored from 1 to 4
4 – Spontaneous
3 – To verbal command
2 – To pain
1 – No eye opening
Verbal Response (V): Scored from 1 to 5
5 – Oriented, converses normally
4 – Confused conversation
3 – Inappropriate words
2 – Incomprehensible sounds
1 – No verbal responseWikipédia, l’encyclopédie libreWikipedia+2Respiratory Therapy Zone+2Wikipédia, l’encyclopédie libre+2Wikipedia
Motor Response (M): Scored from 1 to 6
6 – Obeys commands
5 – Localizes pain
4 – Withdraws from pain
3 – Abnormal flexion (decorticate)
2 – Extension to pain (decerebrate)
1 – No motor responseRespiratory Therapy Zone+12Wikipedia, la enciclopedia libre+12Wikipedia+12
The total GCS score is the sum of these three components, ranging from 3 (deep coma or death) to 15 (fully awake and oriented).
The GCS score helps categorize the severity of a brain injury:
13–15: Mild brain injury
9–12: Moderate brain injury
8 or below: Severe brain injury or coma; often necessitates airway protection measures such as intubation due to the risk of aspiration and inability to maintain airway patency.
For respiratory therapists, a GCS score of 8 or less typically indicates a decreased level of consciousness, which puts the patient at risk for airway obstruction, aspiration, and respiratory failure. In such cases, immediate intervention—often including endotracheal intubation and mechanical ventilation—is required.
The GCS is extensively used in emergency departments, intensive care units, and pre-hospital settings to:
Guide treatment decisions
Track changes in neurological status
Predict patient outcomes
Support airway management decisions, particularly for respiratory therapists
Emergency medical responders use the GCS in the field to quickly assess trauma victims and communicate the severity of injury to receiving hospitals. In intensive care units, the scale helps track a patient’s neurological progression or deterioration over time. It also plays a role in determining prognosis, especially following traumatic brain injuries, strokes, or cardiac arrest.
While the GCS is a valuable assessment tool, it has limitations:
Difficult to assess verbal responses in intubated patients or those with language barriers
May not capture subtle changes in neurological function, especially in focal brain injuries
Standard GCS may not be appropriate for pediatric populations; a modified Pediatric Glasgow Coma Scale is used instead
In pediatric populations, especially infants and toddlers, the standard GCS may not be appropriate due to developmental differences in communication and motor skills. In these cases, a modified version of the scale known as the Pediatric Glasgow Coma Scale is used, which adjusts scoring criteria to better reflect age-appropriate responses.
To reinforce your understanding of the Glasgow Coma Scale, consider the following practice questions:
What are the three categories evaluated in the Glasgow Coma Scale (GCS)?
Best Eye Response, Best Verbal Response, and Best Motor Response
A score of 4 in Best Eye Response indicates:
The patient’s eyes open spontaneously
A score of 5 in Best Verbal Response indicates:
The patient is oriented to person, place, and time
A score of 6 in Best Motor Response indicates:
The patient obeys commands
An overall GCS score of 8 or less indicates:
Severe brain injury; the patient is comatose and requires airway protection
